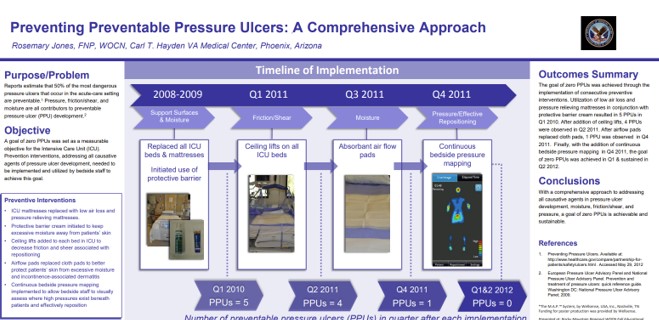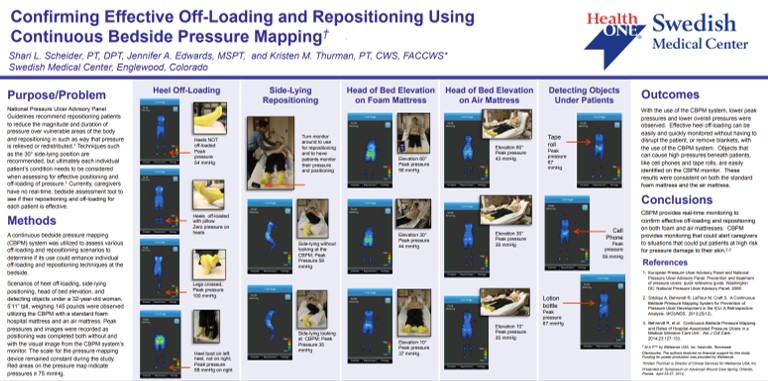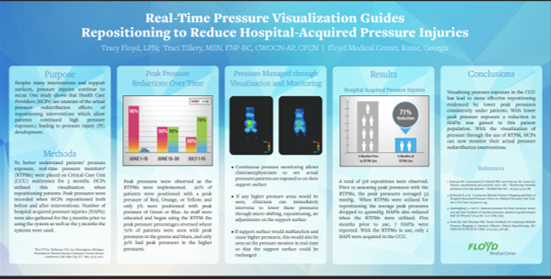
This real-world clinical poster from Floyd Medical Center shows that using a real-time pressure visualization monitor led to a 71% reduction in hospital-acquired pressure injuries (HAPIs) over 5 months in the critical care unit, by guiding staff to reposition patients more effectively and reduce peak pressure exposures.