With the use of real-time pressure mapping feedback, student nurses were able to significantly reduce interface pressure compared to repositioning without the system, demonstrating its value in teaching effective pressure ulcer prevention.
With the use of real-time pressure mapping feedback, student nurses were able to significantly reduce interface pressure compared to repositioning without the system, demonstrating its value in teaching effective pressure ulcer prevention.
This clinical article from American Nurse explains that pressure mapping provides visual, real-time information on pressure distribution, allowing clinicians to see high-pressure areas and verify whether repositioning and support surface interventions are actually relieving pressure, rather than relying solely on skin assessment or patient feedback.

These Japanese Dermatological Association guidelines state that pressure injury prevention depends on confirming actual interface pressure. They direct caregivers to check sacral pressure with an interface pressure meter, reinforcing that effective repositioning must be guided by measured pressure rather than routine practice.
These guidelines reinforce a workflow principle: repositioning should be verified with objective interface pressure measurement. They direct caregivers to check sacral pressure with an interface pressure meter, moving practice from routine turning to measured confirmation.
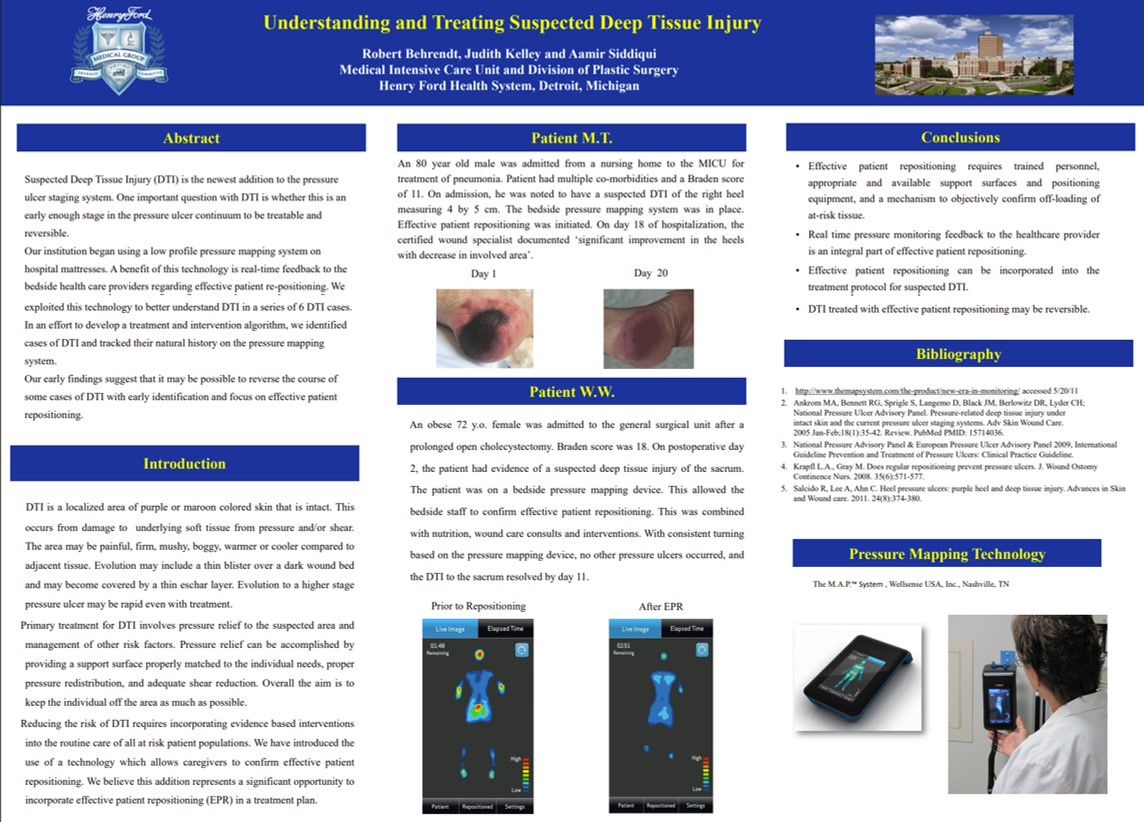
A Henry Ford Hospital elderly patient presented with a deep tissue injury (DTI), which was fully resolved within 11 days using real-time pressure monitoring, with no additional ulcers developing.
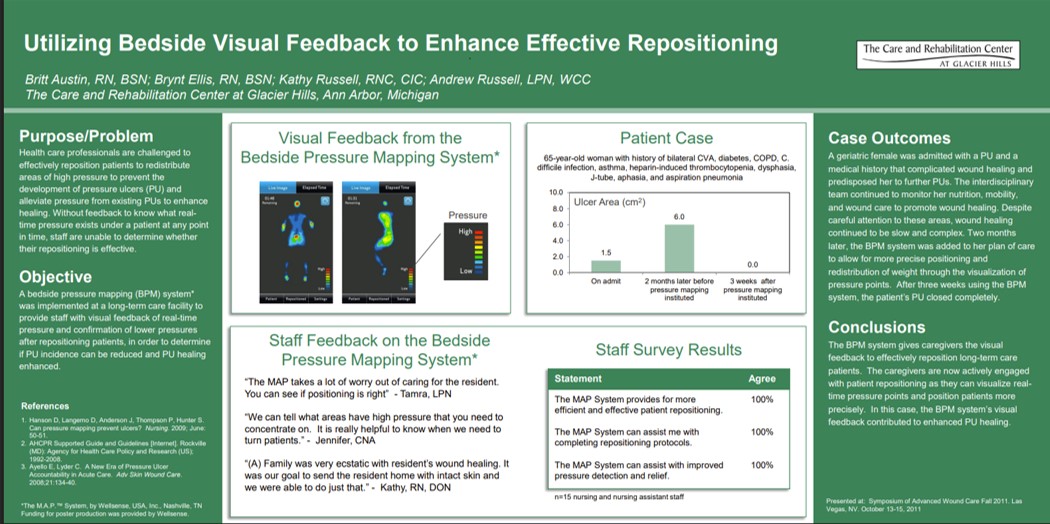
A 65-year-old long-term care patient at Glacier Hills with a non-healing pressure ulcer achieved complete wound closure within 3 weeks after the introduction of real-time bedside pressure visualization to guide repositioning.
This study from NYU School of Medicine found Stage IV pressure ulcers cost about $125k–$129k per patient in hospital treatment costs when ulcer-related complications were included. These costs are far higher than prior estimates and emphasize early recognition and treatment to stop progression to Stage IV and avoid extreme, non-reimbursed “never event” costs.
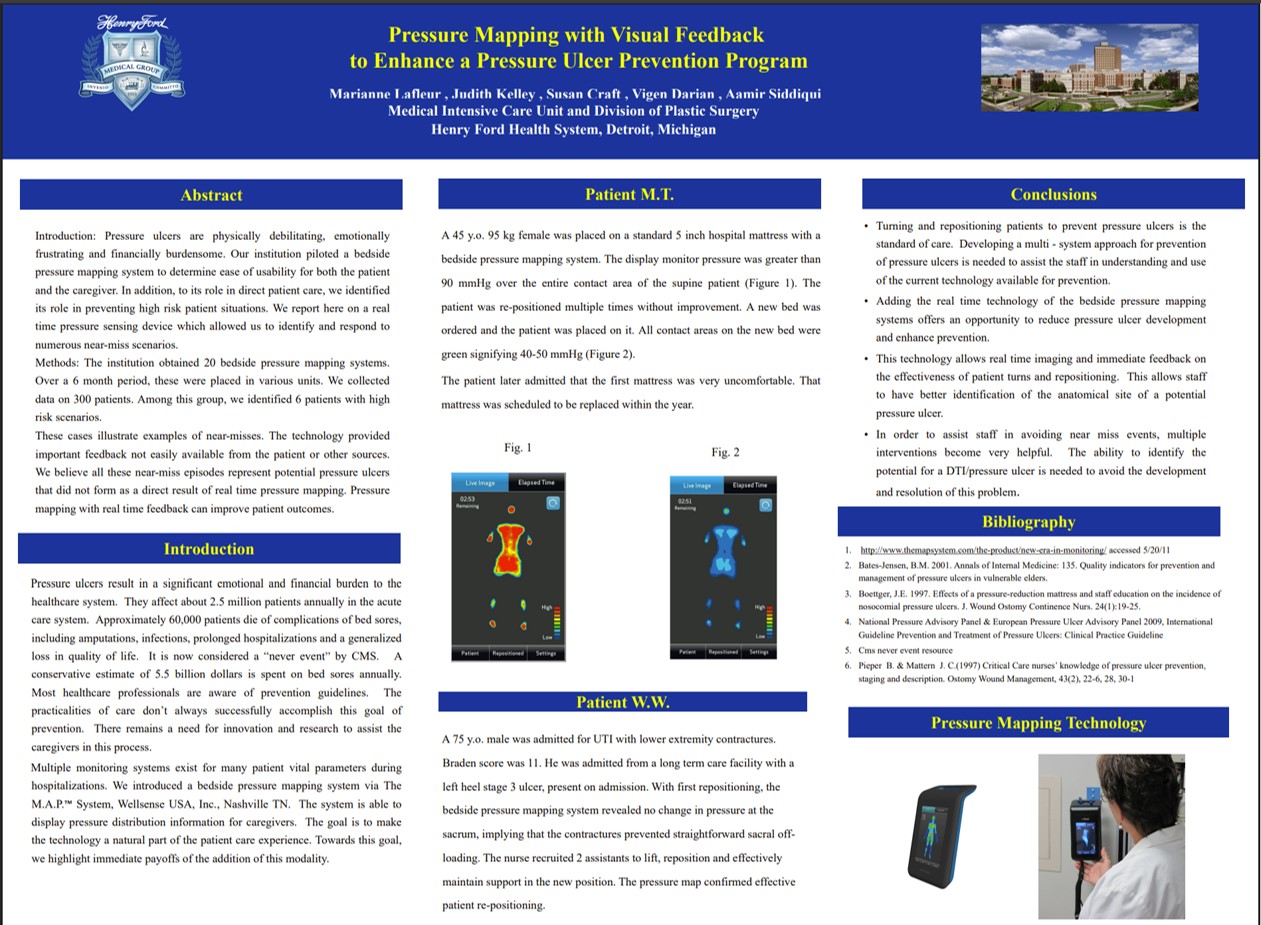
Henry Ford Health System utilized real-time pressure mapping with visual feedback to enhance pressure ulcer prevention, confirming effective repositioning for patients and gaining acceptance from caregivers and patients. The technology showed immediate benefits in identifying and adjusting patient positions to prevent ulcer development.

“In a VA study of veterans with spinal cord injury, the presence of a pressure injury increased average health care costs by $77,587 compared to those without, driven by higher inpatient costs, emphasizing the need for prevention.”
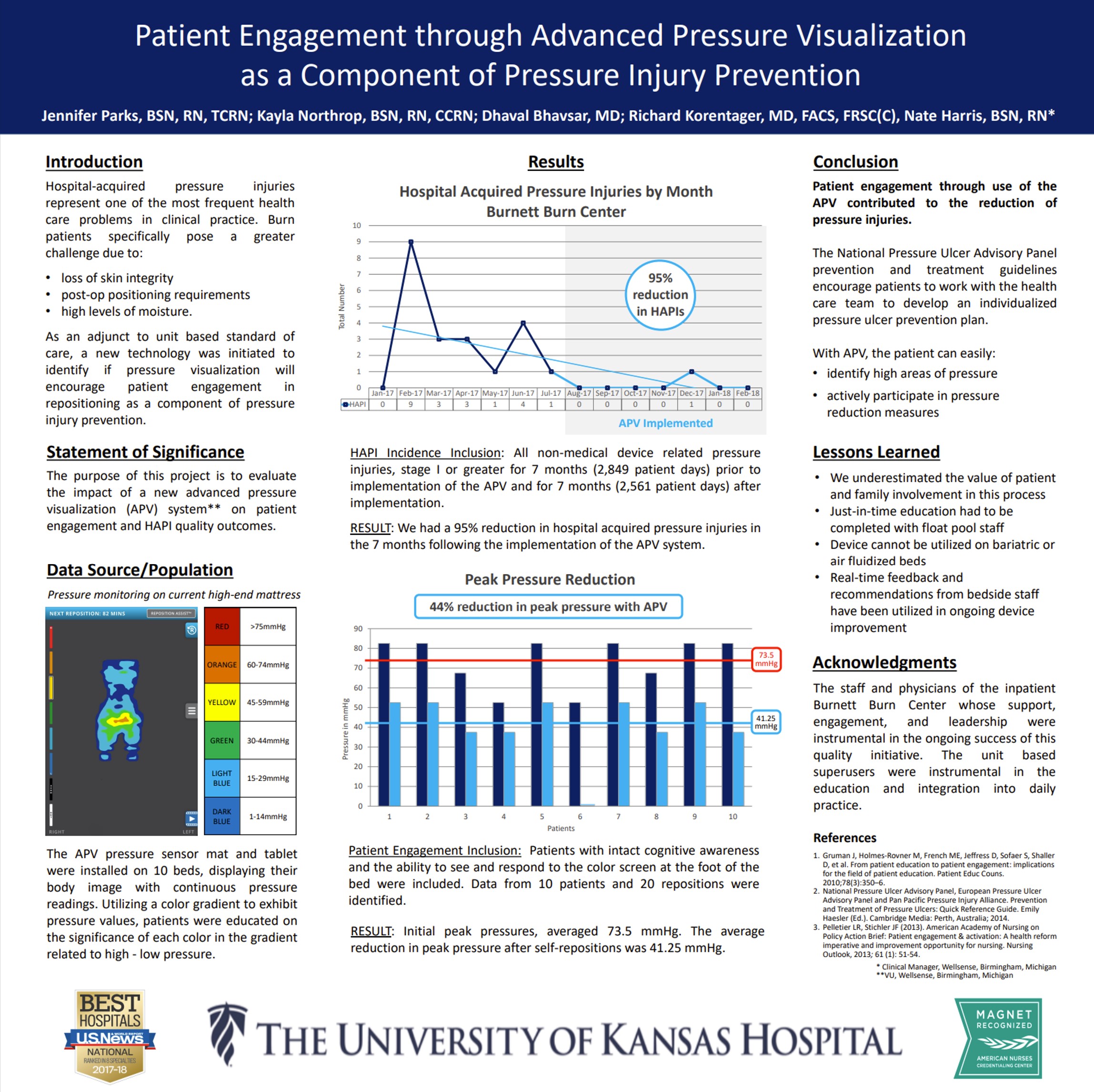
This study frames pressure visualization as a patient-facing tool: by making pressure visible, it motivates participation and supports behavior change around repositioning. The work reinforces that engagement improves when patients can see the cause-and-effect of their own movement on pressure.